Whiplash – a pain in the neck…
%22%20transform%3D%22translate(.6%20.6)%20scale(1.14453)%22%20fill-opacity%3D%22.5%22%3E%3Cellipse%20fill%3D%22%23f6ffff%22%20rx%3D%221%22%20ry%3D%221%22%20transform%3D%22matrix(6.4644%20-50.46248%20118.47457%2015.17694%20214.3%2052)%22%2F%3E%3Cellipse%20cx%3D%2296%22%20cy%3D%22153%22%20rx%3D%22217%22%20ry%3D%2229%22%2F%3E%3Cellipse%20fill%3D%22%23192322%22%20rx%3D%221%22%20ry%3D%221%22%20transform%3D%22matrix(13.4201%2032.08177%20-63.82464%2026.69842%2028.4%2020.8)%22%2F%3E%3Cellipse%20fill%3D%22%23de7a7a%22%20rx%3D%221%22%20ry%3D%221%22%20transform%3D%22matrix(-7.22597%20-48.35007%2044.43893%20-6.64144%2083.8%2090.8)%22%2F%3E%3C%2Fg%3E%3C%2Fsvg%3E) What is it?
What is it?
 What is it?
What is it?Whiplash is a type of neck injury caused by sudden movement of the head forwards, backwards or sideways (1).
Most cases of whiplash injury occur in car accidents, however any incident that results in a sharp movement of the head can generate the same set of symptoms, other common causes include;
- a sudden blow to the head – for example, during sports such as boxing or rugby
- a slip or fall where the head is suddenly jolted backwards
- being struck on the head by a heavy or solid object (1).
A more formal definition of whiplash is ‘An acceleration deceleration mechanism of energy transfer to the neck. It may result from rear-end or side-impact motor-vehicle collisions, but can also occur during diving or other mishaps. The impact may result in bony or soft tissue injuries, which in turn may lead to a variety of clinical manifestations’ (2). Most people will either have had an episode of whiplash, or will know someone who has had it, given that it is so common it may surprise you to know that the knowledge base for its treatment is considered ‘incomplete’ (3).
%22%20transform%3D%22translate(.8%20.8)%20scale(1.5625)%22%20fill-opacity%3D%22.5%22%3E%3Cellipse%20fill%3D%22%23fff%22%20rx%3D%221%22%20ry%3D%221%22%20transform%3D%22matrix(-29.26405%20-3.77321%209.08584%20-70.46746%20146.6%20112)%22%2F%3E%3Cellipse%20fill%3D%22%23fff%22%20rx%3D%221%22%20ry%3D%221%22%20transform%3D%22matrix(4.30679%20-75.32502%2027.16959%201.55345%20149.3%20117.2)%22%2F%3E%3Cellipse%20fill%3D%22%23fff%22%20cx%3D%22145%22%20cy%3D%22118%22%20rx%3D%2229%22%20ry%3D%2266%22%2F%3E%3Cellipse%20fill%3D%22%23dcdcdc%22%20cx%3D%2236%22%20cy%3D%2272%22%20rx%3D%2284%22%20ry%3D%2284%22%2F%3E%3C%2Fg%3E%3C%2Fsvg%3E) What are the symptoms?
What are the symptoms?
 What are the symptoms?
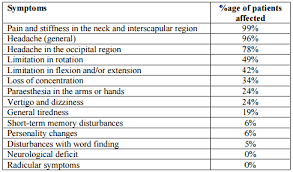
What are the symptoms?The most common symptoms associated with whiplash are neck and shoulder pain and neck stiffness when turning the head. Less commonly there can be pins and needles or numbness in the arms, dizziness and ‘brain fog’ (1). A full list of symptoms and how common they are can be seen below (4).
What causes it?
In a whiplash injury the problem is caused by the head being thrown backwards then forwards very sharply in relation to the shoulders. The severity of the impact will have an impact on what bodily structures are damaged and how bad the damage is. If the impact is relatively light then only the muscles will be damaged as the severity increases damage will be seen in the ligaments, then the joints of the neck, then the brain (5). To give an idea of how little impact is needed to produce large forces in the neck, a 20mph collision will exert a force of up to 12Gs on the neck when it is thrown backwards (6), this is why even if your collision was light you can still experience quite debilitating symptoms.
 The position of the head is also very important in determining the type of injury experienced. For instance, having the head turned to one side will result in the neck joints, the intervertebral discs and the ligaments at the base of your skull becoming vulnerable, while reducing the muscular
The position of the head is also very important in determining the type of injury experienced. For instance, having the head turned to one side will result in the neck joints, the intervertebral discs and the ligaments at the base of your skull becoming vulnerable, while reducing the muscular
damage you are likely to experience (6). The risk of whiplash type injuries also increases if you are female (possibly due to having less neck musculature (7)) or the impact is unexpected (8).
What to do if I have a whiplash injury
The first thing to do is to report to a health professional for a full assessment, if it has been a road accident or a significant trauma then this may be carried out by a paramedic, however, as some symptoms take hours or days to become apparent, you should go to your GP as soon as the symptoms appear. Unless there are symptoms that would indicate a serious injury (losing consciousness, loss of sensation in the fingers or toes, balance or co-ordination problems) they will usually not require any further investigations such has X-rays or MRIs (9).
What if I continue to have pain?
Even if there is no ‘serious’ injury, a lot of people continue to have pain in the short and the medium term. Most people with whiplash will have their symptoms resolve within 6 months if they receive a care programme from a manual therapist such as an osteopath that includes;
- manual therapy, such as gentle neck mobilisation.
- instruction on how to self-mobilise the neck
- education on how whiplash may affect them (10, 11)
The use of soft collars to prevent neck movement are not considered useful when compared to the correct exercise prescription, so even though they seem like a good idea in the short term they are best avoided (12).
For some people, the pain may persist beyond 6 months, this is called chronic whiplash and may be associated with negative thought about the pain, the incident that caused it and if it will get better (13). For chronic whiplash, properly prescribed exercise combined with education about the pain has been shown to be helpful.
%22%20transform%3D%22translate(.6%20.6)%20scale(1.17969)%22%20fill-opacity%3D%22.5%22%3E%3Cellipse%20fill%3D%22%23fff%22%20rx%3D%221%22%20ry%3D%221%22%20transform%3D%22rotate(-107.7%2035.8%202.9)%20scale(48.55203%20119.2031)%22%2F%3E%3Cellipse%20fill%3D%22%238e524a%22%20cx%3D%22131%22%20cy%3D%22113%22%20rx%3D%2267%22%20ry%3D%2239%22%2F%3E%3Cellipse%20fill%3D%22%23da803c%22%20rx%3D%221%22%20ry%3D%221%22%20transform%3D%22rotate(64.1%20-102%2094.2)%20scale(31.32536%20107.42055)%22%2F%3E%3Cellipse%20fill%3D%22%23fff%22%20cx%3D%2221%22%20cy%3D%2216%22%20rx%3D%2254%22%20ry%3D%2254%22%2F%3E%3C%2Fg%3E%3C%2Fsvg%3E) What is our experience as osteopaths?
What is our experience as osteopaths?
 What is our experience as osteopaths?
What is our experience as osteopaths?At Align Body Clinic we see many people suffering from whiplash (after they have been assessed by their doctor), either acute or chronic who have been struggling with pain and loss of movement. Very commonly we find chronic muscle strains in the neck and upper back alongside neck and upper back joints with restricted motion, which although not serious can be quite debilitating. Each person has unique symptoms, however with some focused massage techniques, joint mobilisation, and tailored exercises we find nearly all of our patients get rid of their symptoms after a course of treatment.
Do you want to know what is causing your pain and if we can help? Why not take advantage of our new patient assessment introductory offer to get you started towards a tailor made recovery plan for only £19.
Are you in a lot of pain and want to get better as soon as possible? If so then why not book in for a new patient consultation, with treatment on the day, for £75.
We are also there to help you from home. Take a look at our suite of exercise resources and advice sheets which you can easily download and use from home.
References
1 – NHS Choices (2016). Whiplash, available at; http://www.nhs.uk/conditions/whiplash/Pages/Introduction.aspx.
2 – Spitzer WO, Skovron ML, Salmi LR, Cassidy JD, Duranceau J, Suissa S, Zeiss E. (1995). Scientific monograph of the Quebec Task Force on Whiplash-Associated Disorders: redefining “whiplash” and its management. Spine, Apr;20(8 Suppl):1S-73S.
3- Gunzberg R, Szpalski M. (1997). Whiplash injuries. Current concepts in prevention, diagnosis, and treatment of the cervical whiplash syndrome. London: Lippincott Williams & Wilkins.
4 – Ronnen HR, de Korte PJ, Brink PR, van der Bijl HJ, Tonino AJ, Franke CL, (1996). Acute whiplash injury: is there a role for MR imaging? – a prospective study of 100 patients. Radiology, Oct;201(1):93-6.
5 – Kumar S, Narayan Y, Amell T, (2002). An electromyographic study of low-velocity rear-end impacts. Spine, May;27(10):1044-55.
6 – Kumar S, Ferrari R, Narayan Y, (2005). Cervical muscle response to head rotation in whiplash-type left lateral impacts. Spine, Mar 1. 30(5):536-41.
7 -Otremski I, Marsh JL, Wilde BR, McLardy Smith PD, Newman RJ, (1989). Soft tissue cervical spinal injuries in motor vehicle accidents. Injury, Nov;20(6):349-51.
8 – Siegmund GP, Sanderson DJ, Myers BS, et al, (2003). Awareness affects the response of human subjects exposed to a single whiplash-like perturbation. Spine, Apr 1. 28(7):671-9.
9 – NICE (2015). Neck Pain – whiplash injury. Clinical Knowledge Summary. Available at; http://cks.nice.org.uk/neck-pain-whiplash-injury#!topicsummary.
10 – Vendrig A, et al. (2000). Results of a multimodal treatment program for patients with chronic symptoms after a whiplash injury of the neck. Spine, 25 (2): p.238–244 (4).
11- Bronfort et al (2010). Effectiveness of manual therapies: the UK evidence report. Chiropractic and Osteopathy, 18:3. Available at; http://chiromt.biomedcentral.com/articles/10.1186/1746-1340-18-3.
12 – Teasell RW. Et al, (2010). A research synthesis of therapeutic interventions for whiplash-associated disorder (WAD): Part 2 – interventions for acute WAD. Pain Res Manage; 15(5):295-304.
13- Seferiadis A. et al. (2004). A review of treatment interventions in whiplash-associated disorders, Eur Spine J, 13 : 387–397