What causes ‘the click’ when I visit an osteopath?
 Joint manipulation, or ‘that clicky thing’, is commonly used by osteopaths and is intended to restore movement to joints all over the body (1). If you have been to see us at Align Body
Joint manipulation, or ‘that clicky thing’, is commonly used by osteopaths and is intended to restore movement to joints all over the body (1). If you have been to see us at Align Body
Clinic, you might know what we mean by ‘the clicky thing’, if you don’t then you can see an example here. Typically a manipulation technique is performed by applying a speedy movement to a specific joint that has been carefully placed in a precise position, this skill takes a combination of anatomical knowledge and practise……lots of practise…. How manipulation may produce a therapeutic benefit is still hotly contested, with opinions including an inhibition of contracted muscles, changes in pain perception, and increasing activation of the muscles surrounding a joint (2). What is fairly clear is that manipulation of a joint produces an increased amount of movement in a joint for a period of time, allowing a ‘window of opportunity’ for the person to begin to move more effectively (either through normal activity or prescribed exercises) (3). This is why when you attend our clinic for treatment, we will recommend exercises and activity to help restore normal function in the days after your appointment.
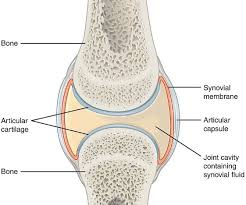
One question we get asked, nearly on a daily basis is ‘what is causing the cracking noise?’, it probably won’t surprise you to know that the answer is not completely clear. When it comes to spinal manipulations as the anatomy of the spine makes the joints being manipulated hard to study. Most of the research in this area has been conducted on the joints of the fingers, and people who ‘crack their knuckles’ (4). A good starting point is what is the structure that the ‘crack’ is happening to? In knuckles the joint affected is the metacarpal phalangeal joint (MCP), which is a synovial joint, meaning it is formed of two bones, a space between the bones that is filled with synovial fluid, and is enclosed by a fibrous capsule (5). One of the earliest studies in this area was in 1947 (6), the researchers looked at MCP joint with radiography and noted that the MCP joint is subjected to force, the following stages have been observed.
The resting phase, no force is being applied, and the joint surfaces are roughly in contact.
In the preliminary phase of separation, the joint surfaces move apart as a small amount of force is used.
As the force gets above a certain threshold, the phase of cracking occurs, and a sound is heard as the joint surfaces move further apart and a clear space appears in the synovial fluid.
The last phase is the refractory period in which the joint cannot be cracked again for about 20 minutes if a force is applied.
 What the authors thought happened was that the formation of the clear space as a result of the rapid movement caused the noise (4). Later research contested this by postulating that the drop in pressure inside the joint created by the sudden increase in space in the joint resulted in gas bubbles being created from vapours that were previously dissolved in the joint fluid (7). The subsequent collapse of the bubbles resulted in the ‘cracking noise’. Although there seems to be a general agreement that there is a bubble formed in the joint after a manipulation, there is still conjecture about what actually causes the noise. Researchers in 2015 used MRI imaging techniques to show that the bubble is still present in the joint after the noise occurs, meaning the collapse of the bubble cannot be the cause of the noise. They have suggested that the chemical change in the fluid when it is subjected to force (tribonucleation) is what causes the noise (8).
What the authors thought happened was that the formation of the clear space as a result of the rapid movement caused the noise (4). Later research contested this by postulating that the drop in pressure inside the joint created by the sudden increase in space in the joint resulted in gas bubbles being created from vapours that were previously dissolved in the joint fluid (7). The subsequent collapse of the bubbles resulted in the ‘cracking noise’. Although there seems to be a general agreement that there is a bubble formed in the joint after a manipulation, there is still conjecture about what actually causes the noise. Researchers in 2015 used MRI imaging techniques to show that the bubble is still present in the joint after the noise occurs, meaning the collapse of the bubble cannot be the cause of the noise. They have suggested that the chemical change in the fluid when it is subjected to force (tribonucleation) is what causes the noise (8).
So, we know that as a result of a force applied to the liquid inside the joint causes a chemical change which (at some point, which point we’re not sure) produces noise. People’s beliefs around the noise are interesting, most patients when asked about what causes the noise during spinal manipulation have inaccurate beliefs (9) such as vertebral repositioning (49%), friction between two vertebrae (23%), with only 9% of people stating the ‘bubble’ reason.
In the same study 40% of people asked thought that the ‘crack’ indicated a successful joint manipulation, which (at the risk of making this entire article redundant) is not true. When measurements of pain change and range of motion are taken from people who have undergone spinal manipulation are compared between people who experienced the ‘crack’ during the manipulation and those who didn’t, the results were the same, indicating that the actual noise from the manipulation is not what produces the observable change (10, 11).
So the next time you attend our clinic, if you receive a manipulation you know that the noise is (probably) a chemical reaction to the movement applied, and that it doesn’t matter if there isn’t a noise!
Do you want to know what is causing your pain and if we can help? Why not take advantage of our new patient assessment introductory offer to get you started towards a tailor made recovery plan for only £19.
Are you in a lot of pain and want to get better as soon as possible? If so then why not book in for a new patient consultation, with treatment on the day, for £75.
We are also there to help you from home. Take a look at our suite of exercise resources and advice sheets which you can easily download and use from home.
References
1 – Fawkes, C (2012). Audible sounds associated with spinal manipulation – A snap shot summary report.
2- Herzog, W. (2000). Clinical Biomechanics of Spinal Manipulation. Churchill Livingstone, London.
3 – Potter, L McCarthy, C Oldham, J (2005). Physiological effects of spinal manipulation: A review of proposed theories. Physical Therapy Reviews 10(3):163-170
4 – Rizvi, A. Loukas, M. Oskouian, R. Shane Tubbs, R. (2018) Let’s Get a Hand on this: Review of the Clinical Anatomy of ‘Knuckle Cracking’. Clinical Anatomy · August 2018. DOI: 10.1002/ca.23243
5 – Snell, R. et al (2008). Clinical Anatomy by Regions (8th edition). Lippincott, Williams and Wilkins, Baltimore.
6 – Roston JB, Haines RW. (1947). Cracking in the metacarpo-phalangeal joint. J Anat 81:165–73.
7- Unsworth A, Dowson D, Wright V. (1971). Cracking joints‘ A bioengineering study of cavitation in the metacarpophalangeal joint. Ann Rheum Dis 30:348–358.
8 – Kawchuk GN, Fryer J, Jaremko JL, Zeng H, Rowe L, Thompson R. (2015). Real-Time Visualization of Joint Cavitation. PLoS ONE 10: e0119470.