How to quickly get rid of plantar fasciitis

If you have ever had the misfortune to have plantar fasciitis you will know that it can be a pervasive problem in that it affects every activity that involves standing or walking. Around 80% of all cases will resolve within one year (even without treatment) but 10% of people will endure the condition for their lifetime (1). Most people have heard of it and many people will have a story about how hard it was to get rid of it, but what exactly happens to the foot when you get plantar fasciitis, and what is the quickest way to get rid of it?
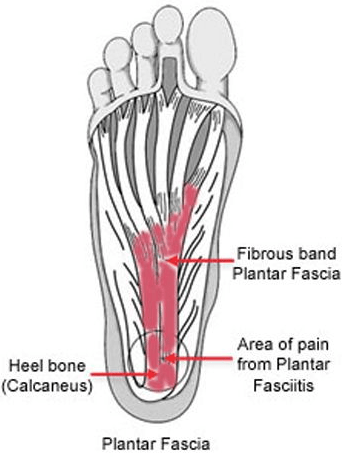 Plantar fasciitis is defined as being ‘a condition in which there is persistent pain associated with chronic degenerative and reparative processes affecting the origin of the plantar fascia and surrounding peri-fascial surfaces’ (1). Sufferers tend to complain of pain on the sole of the foot, usually from the heel and then inwards towards the arch of the foot, the pain is commonly worse on standing first thing in the morning, the pain may lessen as more steps are taken but will reoccur as the activity is prolonged, leading to a limited ability to perform activity (2). You are more likely to get plantar fasciitis if you;
Plantar fasciitis is defined as being ‘a condition in which there is persistent pain associated with chronic degenerative and reparative processes affecting the origin of the plantar fascia and surrounding peri-fascial surfaces’ (1). Sufferers tend to complain of pain on the sole of the foot, usually from the heel and then inwards towards the arch of the foot, the pain is commonly worse on standing first thing in the morning, the pain may lessen as more steps are taken but will reoccur as the activity is prolonged, leading to a limited ability to perform activity (2). You are more likely to get plantar fasciitis if you;
- Are aged 40-60.
- Are female, women are slightly more likely to get it than men.
- Are overweight.
- If you stand for long periods on hard surfaces.
- If you are a runner, or play high impact sports on a hard surface such as basketball (3).
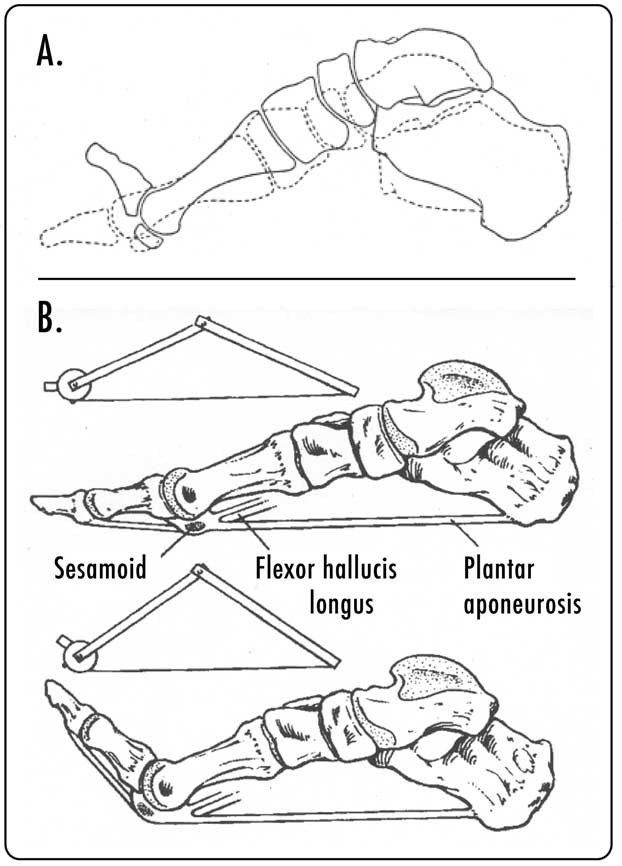 The tissue affected is the plantar fascia, this tough piece of connective tissue runs from the heel bone to the base of the toes and provides shock absorption and when loaded provides a stiffening mechanism that supports the arch of the foot. It is incredibly strong and is thought to be weakest where it inserts into the heel (4). When you walk, at the ‘push off’ phase of the stride the toes have to extend, this generates a pull on the plantar fascia resulting in a bracing of the bones of the foot (see image to the left), resulting in reinforcing the mechanical stability of the foot and possibly resulting conserving energy lost by a recoil effect (5).
The tissue affected is the plantar fascia, this tough piece of connective tissue runs from the heel bone to the base of the toes and provides shock absorption and when loaded provides a stiffening mechanism that supports the arch of the foot. It is incredibly strong and is thought to be weakest where it inserts into the heel (4). When you walk, at the ‘push off’ phase of the stride the toes have to extend, this generates a pull on the plantar fascia resulting in a bracing of the bones of the foot (see image to the left), resulting in reinforcing the mechanical stability of the foot and possibly resulting conserving energy lost by a recoil effect (5).
When the plantar fascia is mechanically overloaded ‘microtears’ are caused where it joins the heel, producing pain and changes in the tendon that might result in the problem becoming chronic (6).
So if you have this pain, how do you get rid of it?
 In some cases the cause of the problem will be obvious, usually the sufferer has done more activity than they are used to, either for a longer duration or more frequently, resulting in damage to the plantar fascia. Resting and reducing the load on the fascia through reducing the intensity, duration and frequency of the activity will often result in a speedy reduction in symptoms. In the short term applying ice to the area of pain and taking anti-inflammatories will help control the pain while recovering (7).
In some cases the cause of the problem will be obvious, usually the sufferer has done more activity than they are used to, either for a longer duration or more frequently, resulting in damage to the plantar fascia. Resting and reducing the load on the fascia through reducing the intensity, duration and frequency of the activity will often result in a speedy reduction in symptoms. In the short term applying ice to the area of pain and taking anti-inflammatories will help control the pain while recovering (7).
For those people who find that they do not recover with rest, there are several possible avenues of investigation that may help them find a solution to their pain.
The first plan of action should be to look at the reasons why the problem occurred in the first place, recent studies have found that sufferers of plantar fasciitis were more likely to have;
- Reduced mobility in the ankle and big toe (8).
- Have a higher body mass index (8).
- Reduced calf strength (8).
- Less flexible hamstrings (8).
- Have recently (if they run) changed their training pace or increased their mileage, or have tried to change to a different foot strike pattern (8, 9).
- Have reduced strength in muscles that flex to toes and turn the ankle out (10).
Being proactive and getting an assessment from an expert to see if any of these features are contributing to your pain so you can quickly take action to correct them will often produce a speedy improvement in your symptoms.
 Other interventions that can make a near-instant impact include;
Other interventions that can make a near-instant impact include;
- Plantar fascia-specific stretches, usually ankle stretches that also extend the toes (11).
- Progressive loading of the plantar fascia over a course of 12 weeks, using strength exercises that specifically load the plantar fascia (12).
- Recent reviews have shown that shoe inserts (orthotics) that raise the heel up and decrease the tension on the plantar fascia may reduce the pain (13). It is also not important if the inserts are custom made of off the shelf, both are effective (14).
There was also a study that provided strong evidence that carefully prescribed exercise, combined with a course of corticosteroid injections, and activity management over three months produced excellent short and long-term results indicating this may be the most effective non-surgical care option (15).
In our experience as osteopaths to improve the symptoms of plantar fasciitis, we find that an accurate assessment that includes a thorough exercise history, strength tests and joint assessments to determine the cause of the plantar pain is crucial. Using that information we are able to recommend exercise modification, carefully prescribed exercises, and hands-on treatment to quickly get you out of pain.
Our osteopaths at Align Body Clinic in Bath have helped hundreds of people get rid of their plantar fasciitis so they can enjoy life to the full again.
Do you want to know what is causing your pain and if we can help? Why not take advantage of our new patient assessment introductory offer to get you started towards a tailor-made recovery plan for only £19.
Are you in a lot of pain and want to get better as soon as possible? If so then why not book in for a new patient consultation, with treatment on the day, for £75.
You can find a basic stretch and exercise guide to help with the symptoms of plantar fasciitis on our resources page.
References
- Neufeld,S.K. (2008) Plantar fasciitis: evaluation and treatment. Journal of the American Academy of Orthopaedic Surgeons. 16(6), 338-346.
- Souza, T. (2009). Differential Diagnosis and Management for the Chiropractor. 4th ed, Jones and Bartlett, Sudbury.
- Carnes, M, & Vizniak, N. (2011). Conditions Manual. Professional Health Systems, Canada.
- Arangio,G. A, Chen, C. Kim, W. (1997). “Effect of cutting the plantar fascia on mechanical properties of the foot”. Clinical Orthopaedics and Related Research (339): 227–231.
- Gefen, A. 2003). “The in vivo elastic properties of the plantar fascia during the contact phase of walking”. Foot & Ankle International. 24 (3): 238–244.
- Karabay N, Toros T, Hurel C. (2007). Ultrasonographic evaluation in plantar fasciitis. J Foot Ankle Surg, 46(6):442–446.
- Donley, B. Moore, T. Sferra, J. Gozdanovic, J. Smith, R. (2007). The efficacy of oral nonsteroidal anti-inflammatory medication (NSAID) in the treatment of plantar fasciitis: a randomized, prospective, placebo-controlled study. Foot Ankle Int, 28(1):20–23.
- van Leeuwen, B. Rogers, J. Winzenberg, T. et al (2016). Higher body mass index is associated with plantar fasciopathy/‘plantar fasciitis’: systematic review and meta-analysis of various clinical and imaging risk factors Br J Sports Med;50:972-981.
- Nielsen, R. Nohr, E. Rasmussen, S,. Sørensen, H. (2013). Classifying running-related injuries based upon etiology, with emphasis on volume and pace. Int J Sports Phys Ther; Apr;8(2):172-9.
- Sullivan, J., Burns, J., Adams, R., Pappas, E., & Crosbie, J. (2015). Musculoskeletal and Activity-Related Factors Associated With Plantar Heel Pain. Foot & Ankle International, 36(1), 37–45.
- DiGiovanni, F. et al (2003). Tissue-specific plantar fascia-stretching exercise enhances outcomes in patients with chronic heel pain. A prospective, randomized study. J Bone Joint Surg Am. 2003 Jul;85-A(7):1270-7.
- Rathleff, M. S., Mølgaard, C. M., Fredberg, U. , Kaalund, S. , Andersen, K. B., Jensen, T. T., Aaskov, S. and Olesen, J. L. (2015), HL strength training and plantar fasciitis. Scand J Med Sci Sports, 25: e292-e300.
- Lee, S. , McKeon, P. Hertel, J. (2009). Does the use of orthoses improve self-reported pain and function measures in patients with plantar fasciitis? A meta-analysis. Phys Ther Sport; 10(1):12–18.
- Hawke, F. Burns, J. Radford, J. du Toit, V. (2008). Custom-made foot orthoses for the treatment of foot pain. Cochrane Database Syst Rev;(3):CD006801.
- Johannsen, F.E., Herzog, R.B., Malmgaard-Clausen, N.M. et al. (2019). Knee Surgery, Sports Traumatology, Arthroscopy, January 2019, Volume 27, Issue 1, pp 5–12