Can you fix flat feet?

 Flat feet, or to give them their medical name, pes planus, is a common foot condition that is characterized by the inner arch of the foot coming closer to the ground, or even being in contact with the ground. Historically, it was seen as something to be corrected, and if present, it can affect the biomechanics of the legs and back, but how much of a problem is it? Does it need to be corrected? And if so, how would you go about correcting flat feet?
Flat feet, or to give them their medical name, pes planus, is a common foot condition that is characterized by the inner arch of the foot coming closer to the ground, or even being in contact with the ground. Historically, it was seen as something to be corrected, and if present, it can affect the biomechanics of the legs and back, but how much of a problem is it? Does it need to be corrected? And if so, how would you go about correcting flat feet?
What are flat feet?
The arch of the foot is supported by the tough ligaments, tendons, and tissues of the underside of the foot. This arch functions as a shock absorber to help dissipate the forces generated by walking and running (1). With people who have flat feet, these supporting structures are not maintaining the arch, leading to a bone called the navicular moving towards the ground and the heel bone tilting inwards, reducing the arch (2).
Who is more likely to have flat feet?

The short answer here is children! All children are born with flexible flat feet, with a small fat pad protecting the arch during early childhood. Arch development begins around the age of three and can take up to the age of ten to fully develop (3). Between 20% and 37% of the population have some degree of flat footedness (4), and there is a strong genetic link, making it a common feature to be handed down in families (5).
What causes flat feet?
The causes of flat feet are varied and are usually broken down into whether the person was born with it (congenital) or developed it sometime during their life (acquired). There is also a distinction to be made if the foot is flexible or fixed.
Congenital flexible flat feet are where the arch does not develop as described above. This can be an inherited trait, but it can also be due to other genetic factors such as the presence of Down Syndrome, hypermobility conditions such as Ehlers-Danlos or Marfan’s, or differences in how the bones of the foot develop (6).
Congenital rigid flat feet are rare, mainly starting in childhood but can appear at any time of life, and are caused by an increasing union between the tarsal bones resulting in the loss of motion and the arch collapsing (7).
Acquired flat feet are seen when the biomechanics of the foot change to allow the arch to lessen, and the heel bone to tilt inwards. This can be due to trauma, general lack of fitness, periods of inactivity such as after an operation, the hormonal changes seen in pregnancy, or even as a byproduct of being diabetic (8). The arch of the foot is supported by several structures, any of which, if diminished by the factors above, can lead to flat feet.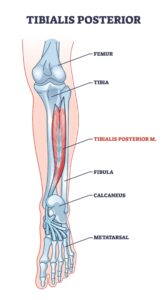
Posterior Tibial Tendon – The tibial tendon arises from a muscle deep in the back of the calf called the Tibialis Posterior. This muscle is primarily responsible for providing dynamic stability to the arch of the foot, and when it contracts it lifts the arch of the foot and reinforces the foot’s rigid structure (9). The tendon can become insufficiently able to perform its task due to trauma, obesity, overuse, or even due to steroid use, the arch will lose its ‘lift’ and eventually result in a flat foot (10). When this happens, the calf muscles change their influence on the foot position from being supporting of the arch to further exacerbating the problem (11).
Plantar Fascia – The Plantar Fascia is a tough, wide band of connective tissue on the sole of the foot. It provides stability to the arch and limits its ‘overstretch’. If this tissue is not able to limit the stretching effect of weight-bearing and walking then the arch can begin to fail, leading to a flat foot (11).
Gluteal Muscles – The gluteal muscles of the hip are involved in outward rotation of the hip joint. Strong gluteal muscles will help keep the hip joint stable so that the knees and the arch of the foot do not collapse inwards; in fact, strong gluteal muscles will help lift the arch (12).
How to fix flat feet
Not all flat feet need to be fixed!
There is no evidence that treating children who have flat feet that are not painful and do not have any underlying condition will make any difference to their functioning (11).
Children who have flat feet with some pain in the foot, leg or back can benefit from orthotics to help support the arch (13).
In rigid flat feet, where the bones of the foot have fused together, the only option is surgery to help restore normal function of the foot. Approaches have been developed that can be applied to various expressions of flat feet in children of various ages (14).
 With acquired flexible flat feet several things can be effective. The first task would be to reduce pain in the foot; this can be achieved with painkillers and advice on supportive or cushioning footwear, or massage and joint mobility techniques to improve movement. It is also crucial to address any underlying factors that contributed to the development of the flat foot, such as if the person is obese or if they are overdoing activity, leading to excessive leg fatigue (15).
With acquired flexible flat feet several things can be effective. The first task would be to reduce pain in the foot; this can be achieved with painkillers and advice on supportive or cushioning footwear, or massage and joint mobility techniques to improve movement. It is also crucial to address any underlying factors that contributed to the development of the flat foot, such as if the person is obese or if they are overdoing activity, leading to excessive leg fatigue (15).
What can also be very effective is exercise therapy for the affected areas. As explained above, if the calf muscles have become very tight due to the change in shape of the foot, then stretching them can be helpful to restore normal motion and reduce pain. Strengthening muscles such as the tibialis posterior and other calf muscles, as well as the plantar fascia, will help restore and stabilise the arch, leading to improved function when weight-bearing (11). Attention should also be given to the function of the core and gluteal muscles to support the function and integrity of the arch of the foot (17).
Do you want to know what is causing your pain and if we can help? Why not take advantage of our new patient assessment introductory offer to get you started towards a tailor-made recovery plan for only £19.
Are you in a lot of pain and want to get better as soon as possible? If so, then why not book in for a new patient consultation, with treatment on the day, for £75.
References
1 – Kelly LA, Cresswell AG, Farris DJ. The energetic behaviour of the human foot across a range of running speeds. Sci Rep. 2018 Jul 12;8(1):10576
2 – Troiano G, Nante N, Citarelli GL. Pes planus and pes cavus in Southern. Annali ell’Istituto Superiore di Sanita. 2017 Jun 7;53(2):142-5.
3 – Squibb M, Sheerin K, Francis P. Measurement of the Developing Foot in Shod and Barefoot Paediatric Populations: A Narrative Review. Children. 2022 May 19;9(5):750.
4 – Munro BJ, Steele JR. Foot-care awareness. A survey of persons aged 65 years and older. J Am Podiatr Med Assoc. 1998 May;88(5):242-8.
5 – Pita-Fernandez S, Gonzalez-Martin C, Alonso-Tajes F, Seoane-Pillado T, Pertega-Diaz S, Perez-Garcia S, Seijo-Bestilleiro R, Balboa-Barreiro V. Flat Foot in a Random Population and its Impact on Quality of Life and Functionality. J Clin Diagn Res. 2017 Apr;11(4):LC22-LC27.
6 – Wilson DJ. Flexible vs Rigid Flat Foot, 2019. Available from: https://www.news-medical.net/health/Flexible-vs-Rigid-Flat-Foot.aspx (Accessed 8 Aug 2025)
7 – Cass AD, Camasta CA. A review of tarsal coalition and pes planovalgus: clinical examination, diagnostic imaging, and surgical planning. J Foot Ankle Surg. 2010 May-Jun;49(3):274-93
8 – Raj MA, Tafti D, Kiel J. Pes Planus. [Updated 2023 May 23]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430802/
9 – Bubra PS, Keighley G, Rateesh S, Carmody D. Posterior tibial tendon dysfunction: an overlooked cause of foot deformity. Journal of family medicine and primary care. 2015 Jan;4(1):26. Available from:https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4367001/
10 – Semple R., Murley G., Woodburn J, Turner D. Tibialis posterior in health and disease: a review of structure and function with specific reference to electromyographic studies.Journal of foot and ankle research 2009; 2: 24.
11 – SM Javad M, Ramin E, Taghi B. Flatfoot in children: how to approach? Iran Journal of Paediatrics.2007. 17(No.2): 163-170.
12 – “Pes Planus.” Physiopedia, . 4 Jan 2024, 07:18 UTC. 15 Sep 2025, 07:09 <https://www.physio-pedia.com/index.php?title=Pes_Planus&oldid=348448>.
13 – Halabchi F, Mazaheri R, Mirshahi M, Abbasian L. Pediatric flexible flatfoot; clinical aspects and algorithmic approach. Iran J Pediatr. 2013 Jun;23(3):247-60
14 – Rodriguez N, Choung DJ, Dobbs MB. Rigid pediatric pes planovalgus: conservative and surgical treatment options. Clin Podiatr Med Surg. 2010 Jan;27(1):79-92.
15 – Vulcano E, Deland JT, Ellis SJ. Approach and treatment of the adult acquired flatfoot deformity. Curr Rev Musculoskelet Med. 2013 Dec;6(4):294-303
16 – Blitz NM, Stabile RJ, Giorgini RJ, DiDomenico LA. Flexible pediatric and adolescent pes planovalgus: conservative and surgical treatment options. Clinics in podiatric medicine and surgery. 2010 Jan 1;27(1):59-77.