What is referred pain?

 Pain is the most common reported symptom in medicine (1). Often, the reason for the pain is obvious, such as a wound or a painful skin infection, but commonly the pain a person feels is a bit more vague, variable, and its source is not obvious; this could be referred pain.
Pain is the most common reported symptom in medicine (1). Often, the reason for the pain is obvious, such as a wound or a painful skin infection, but commonly the pain a person feels is a bit more vague, variable, and its source is not obvious; this could be referred pain.
Referred pain is defined as ‘pain perceived at a location other than the site of the painful stimulus/ origin’. It is generally thought to be the result of how the brain interprets signals from a collection of nerves that are interconnected, leading to confusion around its source (2).
It is important here to differentiate between nociception and pain. Nociception is the detection and transmission of noxious stimuli by nerves called nociceptors; pain is how the higher centres of the brain interpret that nociceptive signal once it is transmitted to the brain. How you perceive pain is a combination of the nociceptive signal and other biological, psychological, and social factors (3). This distinction makes the task of finding the source of referred pain even more difficult!
Why do you get referred pain?
Surprisingly, there is no consensus on what causes referred pain and what the mechanism is that causes it (4). The most commonly cited explanation is that the convergence of nerves in the spine bring unable to differentiate between signals from each nerve in the bundle (1).
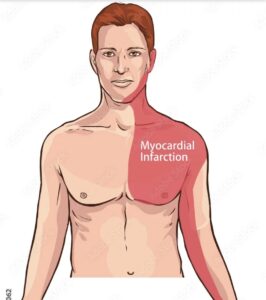
Nerves enter the spine at different levels, and there are several structures in the body that are supplied from each level. For instance, the nerves that originate from the upper back can transmit a nociceptive signal from both your arm and your heart. Once the nerves that individually relay information from either the arm or the heart arrive in the spinal cord, they become part of a common nerve pathway that further feeds the information up the brain. Due to the common nerve pathway, the brain knows that the pain is coming from the nerves that have entered the upper back, but it is unable to detect from exactly which structure. This is why pain from a heart attack is commonly felt in the left arm. (1).
 Another example of referred pain is when spinal structures, such as joints or intervertebral discs of the lower back produce a nociceptive signal, but the pain is felt deep in the tissues of the thighs and legs as they share the same spinal level (2). This is one of the many reasons why the diagnosis of back and leg pain can be complex.
Another example of referred pain is when spinal structures, such as joints or intervertebral discs of the lower back produce a nociceptive signal, but the pain is felt deep in the tissues of the thighs and legs as they share the same spinal level (2). This is one of the many reasons why the diagnosis of back and leg pain can be complex.
How can I tell if my pain is referred?
Identifying referred pain can be tricky, but it has a few features that can usually make it detectable.
What it feels like – referred pain is usually dull, diffuse, or ‘pressure-like’, it will also be hard to localise and can change location.
Can you press on it and make it worse? – If your leg hurts, and you press on the bit of your leg that is sore, and it makes it worse, then it is likely that the sore bit you just pressed on is causing the symptoms. If you try to find referred pain by pressing on the bit that is sore, you won’t be able to exacerbate it.
Professional assessment – Your local friendly osteopath will be able to help diagnose the source of your pain, even if it is referred, by using sensitive tests to provoke the structures that might be causing the pain to be referred. These will differ depending on what the suspected painful structure may be, if the pain is recreated when the test is performed, then there is a reasonable chance the pain is referred (5).
tests to provoke the structures that might be causing the pain to be referred. These will differ depending on what the suspected painful structure may be, if the pain is recreated when the test is performed, then there is a reasonable chance the pain is referred (5).
How do you fix referred pain?
Very simply put, to get rid of referred pain, you must first identify why it is occurring; only by understanding which structure is causing the pain can you then put in place a plan to help. For example, with back and/or leg pain, the pain may be generated from a joint or a disc; the treatment plan for each of these would be very different, so ensuring you have identified the correct referring structure will result in productive treatment.
Are you in a lot of pain and want to get better as soon as possible? If so, then book in for a new patient consultation with treatment.
Not sure we can help with your symptoms? Why not take advantage of our new patient assessment introductory offer to get you started towards a tailor-made recovery plan for only £19.
References
1 – Chen JS, Kandle PF, Murray IV, et al. Physiology, Pain. [Updated 2023 Jul 24]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK539789/
2 – Arendt-Nielsen L, Svensson P .Referred muscle pain: basic and clinical findings. Clin J Pain, 2001, 17 (1): 11–9.
3 – Loeser JD, Melzack R. Pain: an overview. Lancet. 1999 May 08;353(9164):1607-9.
4 – Bogduk N. On the definitions and physiology of back pain, referred pain, and radicular pain. Pain. 2009 Dec 15;147(1-3):17-9
5 – Jin Q, Chang Y, Lu C, Chen L, Wang Y. Referred pain: characteristics, possible mechanisms, and clinical management. Front Neurol. 2023 Jun 28;14:1104817. doi: 10.3389/fneur.2023.1104817. PMID: 37448749; PMCID: PMC10338069.